Oxycodone

Price range: $250.00 through $1,500.00
Oxycodone is a potent opioid painkiller prescribed for severe pain. It works directly on the central nervous system to change how your body perceives and responds to pain. It is available in two primary formulations: short-acting (immediate-release) and long-acting (extended-release).
Drug Class: Opioid Analgesic (Narcotic)
Schedule: Controlled Substance (Schedule II in the US; Class A in the UK; equivalent strict controls in most countries)
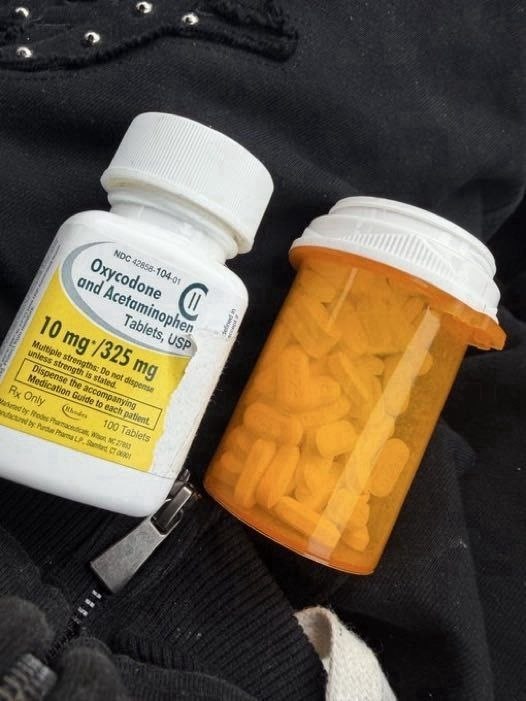
Common Brand Names: OxyContin (extended-release), Roxicodone (immediate-release), OxyIR, Oxyfast, Oxaydo, Xtampza ER
What is Oxycodone?
Oxycodone is a semi-synthetic opioid analgesic derived from thebaine, an alkaloid found in the opium poppy. It was first developed in Germany in 1916 and introduced to the US market in 1939. Today, it is one of the most widely prescribed and also most widely abused prescription opioids in the world.
Oxycodone is classified as a Schedule II / Class A controlled substance due to its high potential for abuse, dependence, addiction, overdose, and death.
Mechanism of Action (Pharmacology)
Oxycodone exerts its effects by binding to and activating mu-opioid receptors (MOR) located primarily in the central nervous system (brain and spinal cord), as well as in peripheral tissues such as the gastrointestinal tract.
When oxycodone binds to these receptors:
-
Pain perception is reduced — the transmission of pain signals from the spinal cord to the brain is inhibited
-
Pain response is altered — the emotional and cognitive processing of pain is changed
-
Dopamine release increases — producing feelings of pleasure, euphoria, and reward (this is the mechanism underlying its abuse potential)
Unlike morphine, oxycodone has higher oral bioavailability (approximately 60-87%), making it effective when taken by mouth.
Medical Uses
Oxycodone is indicated for the management of moderate to severe acute or chronic pain when other non-opioid analgesics (such as acetaminophen, ibuprofen, or naproxen) are inadequate.
Common clinical applications include:
-
Post-surgical pain (e.g., orthopedic, abdominal, or thoracic surgery)
-
Cancer-related pain (moderate to severe)
-
Trauma pain (fractures, burns, injuries)
-
Chronic non-cancer pain (only when benefits clearly outweigh risks — controversial and increasingly restricted)
-
Breakthrough pain in patients already on around-the-clock opioid therapy
Immediate-release formulations are used for acute pain or breakthrough episodes. Extended-release formulations (e.g., OxyContin) are used for around-the-clock management of chronic pain requiring long-term opioid therapy.
Dosage Forms and Strengths
Oxycodone is available in several formulations:
Immediate-release (IR):
-
Capsules: 5 mg
-
Tablets: 5 mg, 10 mg, 15 mg, 20 mg, 30 mg
-
Oral solution (concentrate): 100 mg/5 mL (20 mg/mL) — for opioid-tolerant patients only
-
Oral solution: 5 mg/5 mL
Extended-release (ER):
-
Tablets: 10 mg, 15 mg, 20 mg, 30 mg, 40 mg, 60 mg, 80 mg (OxyContin)
-
Capsules: 9 mg, 13.5 mg, 18 mg, 27 mg, 36 mg (Xtampza ER)
Combination products (with acetaminophen):
-
Percocet: 2.5 mg / 325 mg, 5 mg / 325 mg, 7.5 mg / 325 mg, 10 mg / 325 mg
-
Endocet, Roxicet, others
Typical Dosing (Educational Example Only)
Immediate-release (opioid-naïve adults):
-
Starting dose: 5 to 15 mg every 4 to 6 hours as needed for pain
-
Dose adjustments: Based on pain severity and previous opioid exposure
Extended-release (opioid-tolerant patients only):
-
Starting dose: 10 mg every 12 hours
-
Titrated slowly based on response
⚠️ Important: Extended-release oxycodone is not for opioid-naïve patients and should not be used for acute pain or as-needed dosing. Crushing, chewing, or dissolving extended-release tablets can cause rapid release and fatal overdose.
Contraindications
Oxycodone is contraindicated in patients with:
-
Significant respiratory depression (e.g., COPD exacerbation, asthma attack, pneumonia)
-
Acute or severe bronchial asthma in an unmonitored setting
-
Known or suspected gastrointestinal obstruction (including paralytic ileus)
-
Hypersensitivity to oxycodone or any component of the formulation
-
Concurrent use of monoamine oxidase inhibitors (MAOIs) or within 14 days of MAOI discontinuation
Warnings (Boxed / Black Box Warnings)
The FDA and international regulators require multiple boxed warnings for oxycodone:
1. Addiction, Abuse, and Misuse
Oxycodone exposes patients and other users to the risks of opioid addiction, abuse, and misuse, which can lead to overdose and death. Assess each patient’s risk before prescribing.
2. Life-Threatening Respiratory Depression
Serious, life-threatening, or fatal respiratory depression may occur with oxycodone. Monitor for respiratory depression, especially during initiation and dose titration.
3. Accidental Ingestion
Accidental ingestion of even one dose of oxycodone, especially in children, can result in a fatal overdose.
4. Neonatal Opioid Withdrawal Syndrome (NOWS)
Prolonged use during pregnancy can result in neonatal opioid withdrawal syndrome, which may be life-threatening if not recognized and treated.
5. Interactions with Alcohol or CNS Depressants
Concomitant use with alcohol, benzodiazepines, other opioids, muscle relaxants, or sedating antihistamines can cause profound sedation, respiratory depression, coma, and death.
6. Risks from Concomitant Use with Benzodiazepines or Other CNS Depressants
Reserve concomitant prescribing for use in patients for whom alternative treatment options are inadequate. Limit dosages and durations to the minimum required.
Common Side Effects
Very common (>10%):
-
Constipation
-
Nausea
-
Vomiting
-
Somnolence (drowsiness)
-
Dizziness
-
Headache
-
Pruritus (itching)
Common (1-10%):
-
Dry mouth
-
Sweating
-
Fatigue
-
Weakness
-
Loss of appetite
-
Abdominal pain
-
Diarrhea
Serious (rare but life-threatening):
-
Respiratory depression (slow or shallow breathing)
-
Severe hypotension (low blood pressure)
-
Adrenal insufficiency
-
Serotonin syndrome (when combined with serotonergic drugs)
-
Opioid-induced hyperalgesia (increased pain sensitivity)
-
Androgen deficiency (low testosterone with long-term use)
Dependence, Tolerance, and Withdrawal
Tolerance: Over time, patients require higher doses to achieve the same analgesic effect.
Physical dependence: Abrupt discontinuation or rapid dose reduction causes withdrawal symptoms. This is not the same as addiction.
Withdrawal symptoms include:
-
Agitation, anxiety, insomnia
-
Yawning, tearing, runny nose
-
Sweating, chills, goosebumps
-
Muscle aches, bone pain
-
Nausea, vomiting, diarrhea
-
Dilated pupils, rapid heart rate
-
Hypertension
Addiction (Opioid Use Disorder): A chronic, relapsing brain disease characterized by:
-
Compulsive drug seeking
-
Loss of control over use
-
Continued use despite harm
Tolerance and physical dependence are expected with prolonged opioid therapy. Addiction is a pathological pattern of behavior that requires treatment.
Overdose Signs and Treatment
Signs of opioid overdose:
-
Pinpoint pupils (miosis)
-
Respiratory depression (slow, shallow, or stopped breathing)
-
Extreme drowsiness or unresponsiveness (cannot be woken)
-
Blue or purple lips/fingertips (cyanosis)
-
Cold, clammy skin
-
Slow or absent heartbeat
-
Gurgling or snoring sounds (from airway obstruction)
Emergency treatment:
-
Naloxone (Narcan): An opioid antagonist that rapidly reverses opioid effects
-
Call emergency services immediately (911 or local equivalent)
-
Rescue breathing and CPR as needed
-
Multiple doses of naloxone may be required due to oxycodone’s long duration of action
Drug Interactions (Major)
Oxycodone interacts with many medications, including:
| Drug Class | Interaction | Outcome |
|---|---|---|
| Benzodiazepines (diazepam, alprazolam, lorazepam) | Additive CNS depression | Profound sedation, respiratory depression, death |
| Alcohol | Additive CNS depression | Sedation, coma, death |
| Other opioids (morphine, hydrocodone, fentanyl) | Additive effects | Overdose, respiratory depression |
| Muscle relaxants (cyclobenzaprine, carisoprodol) | Additive CNS depression | Impaired motor function, sedation |
| Antihistamines (diphenhydramine, hydroxyzine) | Additive CNS depression | Extreme drowsiness |
| MAO inhibitors (phenelzine, tranylcypromine) | Serotonin syndrome | Agitation, hyperthermia, rigidity |
| SSRIs / SNRIs (fluoxetine, sertraline, duloxetine) | Increased serotonin | Serotonin syndrome |
| CYP3A4 inhibitors (erythromycin, ketoconazole, grapefruit juice) | Increased oxycodone levels | Overdose risk |
| CYP3A4 inducers (rifampin, carbamazepine, St. John’s wort) | Decreased oxycodone levels | Reduced efficacy, withdrawal |
Storage and Disposal
Storage:
-
Store securely in a locked cabinet out of reach of children and pets
-
Keep at room temperature (15-30°C / 59-86°F)
-
Do not store in bathrooms or other humid environments
Disposal:
-
The FDA recommends immediate disposal down the toilet or sink (flush method) when no drug take-back option is available
-
Alternatively, use an authorized drug take-back program or DEA-registered collector
-
Do not throw in household trash where children, pets, or others may find them
Regulatory and Legal Status by Country
| Country | Classification | Notes |
|---|---|---|
| United States | Schedule II (C-II) | Prescription required; no refills without new prescription; DEA registration required for prescribing and dispensing |
| United Kingdom | Class A (Misuse of Drugs Act 1971) | Prescription required; Schedule 2 controlled drug |
| Canada | Schedule I (CDSA) | Prescription required; strict record-keeping |
| Australia | Schedule 8 (Controlled Drug) | Prescription required; special authority may be needed |
| Germany | Betäubungsmittel (Narcotic) | Special prescription form required |
| France | Stupéfiant (Narcotic) | Prescription with 28-day maximum; secure prescription pad required |
| Japan | Narcotic | Strict import/export controls; special license required |
History and the Opioid Crisis
Oxycodone played a significant role in the opioid epidemic, particularly following the introduction of OxyContin by Purdue Pharma in 1996. Aggressive marketing claimed the extended-release formulation had lower abuse potential — a claim that proved false. Crushing OxyContin tablets destroyed the time-release mechanism, delivering a potentially fatal dose all at once.
The result was a surge in:
-
Prescription opioid misuse
-
Heroin initiation (many users switched from OxyContin to cheaper heroin)
-
Overdose deaths
-
Lawsuits, criminal charges, and the eventual bankruptcy of Purdue Pharma
Today, reformulated OxyContin (2010 onward) is more resistant to crushing, but abuse and diversion remain serious problems. Extended-release oxycodone is now reserved for opioid-tolerant patients with severe chronic pain, and many prescribers limit opioid therapy to cancer or end-of-life pain only.
| Quantity | 60 Pills, 100 Pills, 500 Pills |
|---|
Related products

Benzodiazepines

Antipsychotics

CNS Stimulants

CNS Stimulants

Gabapentinoids

Barbiturates
Controlled Stimulant

Benzodiazepines